AMT-130 – What This Therapy Is and Why It Attracts So Much Attention AMT-130 gene therapy for Huntington’s disease has become one of the most discussed topics in neurology, biotechnology, ...

16Jun

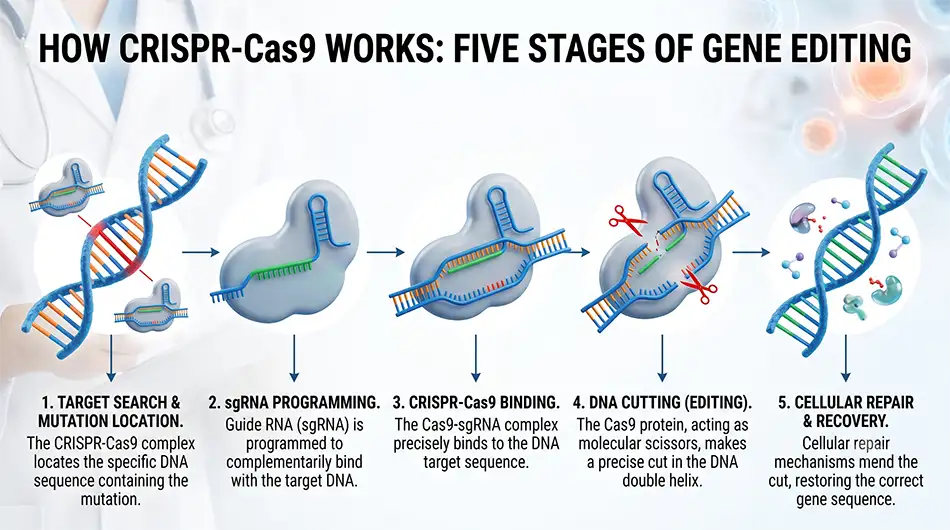
Gene therapy for genetic diseases using CRISPR is aimed not only at reducing symptoms, but at changing the molecular cause of the disease. The name CRISPR is also pronounced as “crisper.” The technology allows finding a specific DNA sequence, turning off a pathological gene, restoring its function, or changing the regulation of another gene.
In pediatrics, this approach is important for hereditary diseases that damage the brain, liver, hematopoietic system, muscles, or visual organs from the earliest years of life. Its application depends on an accurate diagnosis, type of mutation, availability of target cells, and clinical evidence.
To understand how the system works, it can be imagined as a programmable molecular tool. The guide RNA recognizes the target DNA sequence, and the Cas9 protein or another editor performs a change at the specified point. After that, the cell repairs the DNA, and this process is used for therapeutic effect.
The main types of editing differ by the type of change:
The choice of strategy is determined by the specific mutation and tissue biology. One diagnosis may require different editors in different children.
Clinical modes of administration are divided into editing outside the body and directly inside the body. Changes are made to somatic cells, so they should not be passed on to future generations. WHO distinguishes somatic from hereditary genome editing, each subject to different levels of control.
Ex vivo allows testing cells before administration, but requires complex manufacturing and often preparatory chemotherapy. In vivo simplifies access to the liver and certain tissues but increases demands on delivery accuracy.
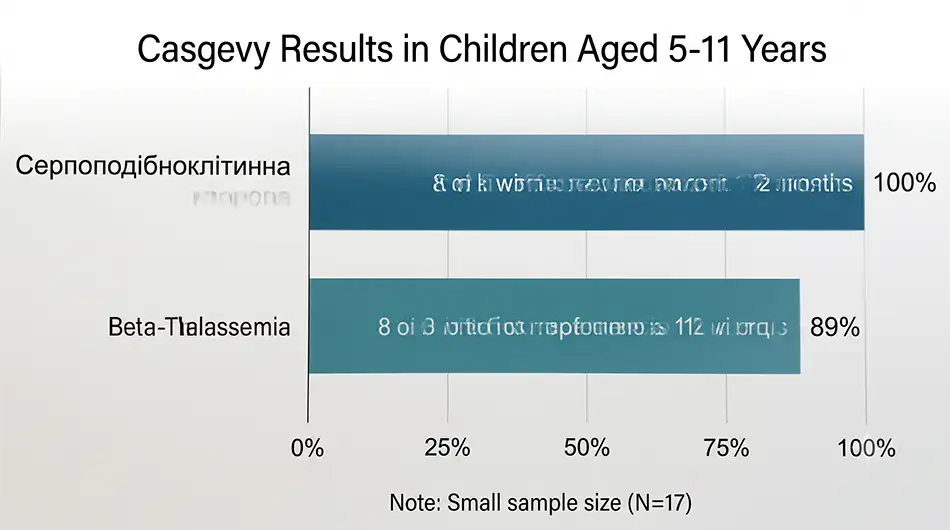
The greatest clinical data accumulation is for hereditary blood diseases. Casgevy uses CRISPR/Cas9 to edit a patient’s own hematopoietic stem cells to increase fetal hemoglobin synthesis. This reduces sickle-shaped erythrocyte deformation and can eliminate the need for regular transfusions in transfusion-dependent beta-thalassemia.
As of July 1, 2026, the FDA expanded Casgevy’s indication in the USA to children from 2 years old with recurrent vaso-occlusive crises or transfusion-dependent beta-thalassemia. In the European Union, EMA indications remain for patients from 12 years old who are eligible for hematopoietic stem cell transplantation and have no suitable familial donor.
FDA pediatric results provide specific guidelines:
These figures apply to small groups and do not guarantee identical results for every child. Duration of effect and long-term safety continue to be evaluated.
In 2025, a team from CHOP and the University of Pennsylvania reported the first systemic personalized base editing for an infant with severe CPS1 deficiency. The disease disrupts ammonia utilization and can quickly cause brain damage. The child received the first dose at 6-7 months of age, after which they were able to consume more protein and reduce the dose of nitrogen excretion medication. No serious adverse events were recorded in initial observations, but long-term monitoring is required.
This case demonstrates an “N-of-1” model, where therapy is designed for a single mutation. It does not prove universal efficacy but shows the possibility of adapting the platform to ultra-rare diseases.
CRISPR is not a standard solution for all hereditary diagnoses. The risk depends on the editor, delivery method, target organ, child’s age, and preparatory treatment.
Before therapy, the team assesses the following factors:
For Casgevy, the FDA notes mucositis, febrile neutropenia, decreased appetite, delayed platelet engraftment, hypersensitivity reactions, and off-target editing risks. Complete myeloablative conditioning is performed before administration, so treatment is only possible in specialized centers.
Due to the possibility of delayed effects, the FDA recommends up to 15 years of monitoring for genome editing products. This is necessary to control the stability of the effect, off-target changes, and late complications.
The pathway starts with molecular confirmation of the diagnosis. The family needs a center experienced in pediatric genetics, the relevant disease, transplantation, or gene therapy.
The practical sequence of actions looks like this:
The decision is made by a multidisciplinary team together with the parents or legal representatives. Participation in a study does not guarantee benefit, and offers of “CRISPR treatment” outside of regulatory-controlled centers require verification.






